Vaccination against rotavirus is currently the most cost-effective and efficient method for preventing rotavirus infections. In 2009, the World Health Organization (WHO) recommended that all countries include oral rotavirus vaccines in their routine immunization programs1. Studies have shown that the currently available rotavirus vaccines are generally safe, although their effectiveness evidence varies across different countries and regions. Overall, rotavirus vaccines demonstrate high efficacy and effectiveness in those developed countries in Europe and the Americas, whereas their performance in developing countries in Africa and Asia remains suboptimal 2-4.
Global Overview of Rotavirus Vaccines
Types of Vaccines
As of now, seven rotavirus vaccines have been approved globally5,6. These include Rotarix (GlaxoSmithKline, Belgium), RotaTeq (Merck & Co., USA), Rotavac (Bharat Biotech, India), Rotasiil (Serum Institute of India), LLR (Lanzhou Institute of Biological Products, China), LLR3 (Lanzhou Institute of Biological Products, China), and Rotavin-M1 (Polyvac, Vietnam). Among these, RotaTeq, Rotarix, Rotavac, and Rotasiil have received WHO prequalification, while LLR, LLR3, and Rotavin-M1 are licensed for use in select countries (Table 4.1). By 2023, Rotarix was being used in 75 countries and RotaTeq in 24 countries; 11 countries introduced both RotaTeq and Rotarix. Additionally, Rotavac was used in 11 countries, Rotasiil in 6 countries, and a combination of Rotasiil and Rotavac in 1 country. Two countries have announced plans to introduce rotavirus vaccines but have not yet specified products7.
Table 4.1 Overview of Current Rotavirus Vaccine Products
| Vaccine | Manufacturer | Serotype/Strain | Year Approved | Immunization Schedule | Dosage/ Form | Intro Country Number |
| Rotarix | GlaxoSmithKline, Belgium | G1P[8] | 2005 | 2 doses, starting at 6 weeks, 4-week interval; completed by 24 weeks | 1.5 mL/dose, liquid | 75 countries |
| RotaTeq | Merck & Co., USA | G1, G2, G3, G4, P[8] | 2006 | 3 doses, starting at 6–12 weeks, 4–10-week interval, completed by 32 weeks | 2 mL/dose, liquid | 24 countries |
| Rotavac | Bharat Biotech, India | G9P[11] | 2014 | 3 doses, starting at 6 weeks, 4-week interval, completed by 8 months | Liquid (frozen and non-frozen) | 11 countries |
| Rotasiil | Serum Institute of India | G1, G2, G3, G4, G9 | 2017 | 3 doses, starting at 6 weeks, 4-week interval, completed within 1 year | 2.5 mL/dose, lyophilized; 2 mL/dose, liquid | 6 countries |
| LLR | Lanzhou Institute of Biological Products, China | G10P[15] | 2000 | 3 doses, starting at 2 months to 3 years, 1 dose annually | 3 mL/dose, liquid | China |
| LLR3 | Lanzhou Institute of Biological Products, China | G2, G3, G4 | 2023 | 3 doses, starting at 6–13 weeks, 1-month interval, 3rd dose by 32 weeks | 2 mL/dose, liquid | China |
| Rotavin-M1 | Polyvac, Vietnam | G1P[8] | 2012 | 2 doses, starting at 6 weeks, completed by 6 months, minimum 1-month interval | 2 mL/dose, liquid (frozen and non-frozen) | Vietnam |
Data Source:Rotavirus Gastroenteritis Expert Consensus Writing Group. Expert consensus on immunoprevention of rotavirus gastroenteritis in children (2024 edition). Chinese Journal of Preventive Medicine. 2024;58(0):1-33.DOI:10.3760/cma.j.cn112150-20231220-00472
He LH, Li JS, Duan ZJ. Progress in research on effectiveness and safety of rotavirus vaccines in China. Chinese Journal of Vaccines and Immunization. 2023;29:239–245. DOI: 10.19914/j.CJVI.2023041
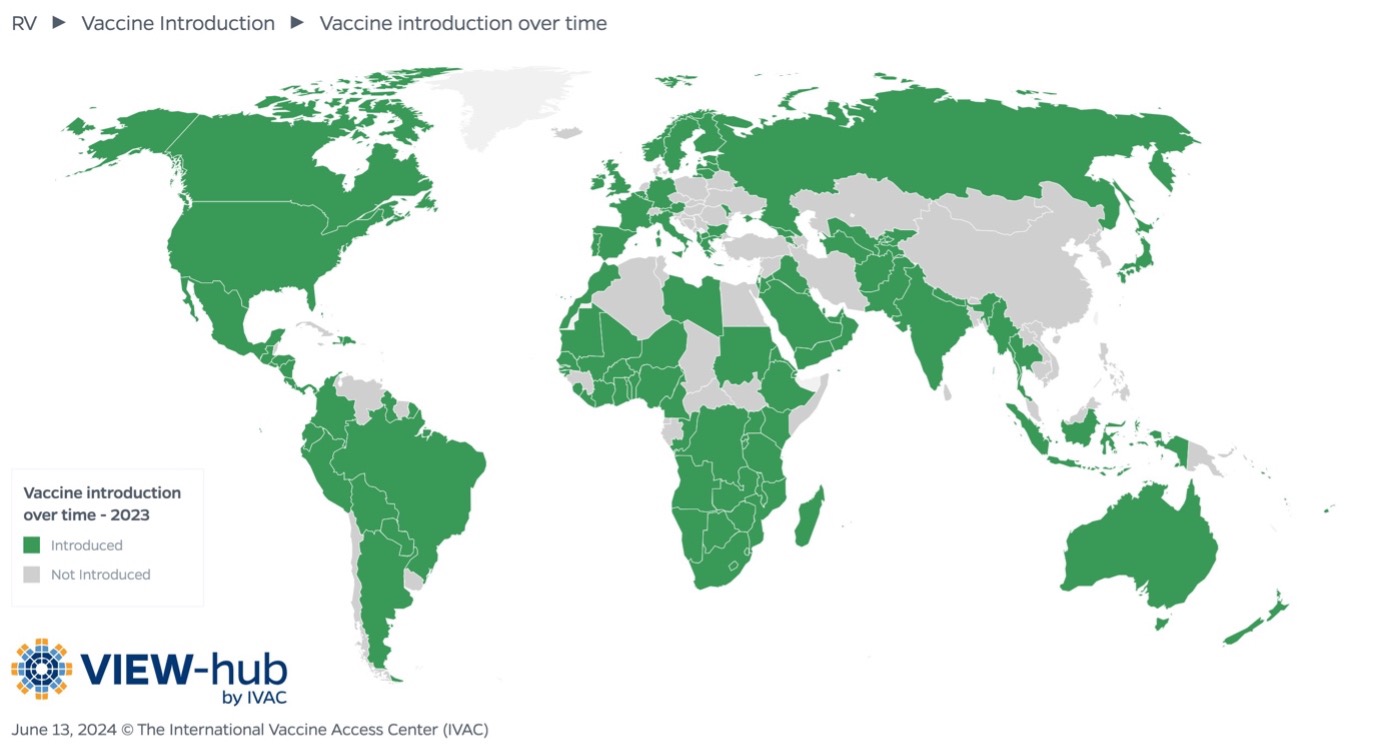
Source: VIEW-hub
Safety, Efficacy, and Effectiveness
Current evidence indicates two widely used rotavirus vaccines’ -Rotarix & RotaTeq- efficacy and effectiveness vary across different countries and regions, which may be attributed to differences in economic levels, lifestyles, genetic backgrounds, and prevalent strains5. All approved Rota vaccine products have demonstrated good safety profiles, without reports of severe adverse events following the immunization12-14,31-33. In general, rotavirus vaccines exhibit higher efficacy and effectiveness in low-mortality regions (primarily the developed countries) compared to high-mortality regions3,4.
The lower effectiveness of RotaTeq in high-mortality regions may be due to several factors: (1) the predominance of the P[6] genotype in some high-mortality regions, which is not covered by RotaTeq; (2) lower economic levels in high-mortality regions, leading to insufficient vaccine coverage as rotavirus vaccination is not included in national immunization programs; and (3) poorer healthcare and nutritional conditions in high-mortality regions, which prolong the course of rotavirus gastroenteritis (RVGE) and increase the severity and mortality of the disease15. Other factors, such as malnutrition (zinc and vitamin A/D deficiencies), gut microbiota, multiple infections, immature infant immune systems, environmental enteropathy, maternal antibodies (via placenta or breast milk), and genetic factors, may also contribute to the varying immunogenicity of rotavirus vaccines across countries16,35. Additionally, the protection of rotavirus vaccine declines more rapidly over time in high-mortality regions17.
Furthermore, evidence suggests that high vaccination coverage among infants and young children can provide herd protection to older populations. This highlights the potential for broader societal benefits as immunization programs are established. Increasing vaccination coverage and continued investment in comprehensive rotavirus vaccination programs may benefit public health and further reduce the clinical and economic burden of the disease30.
Rotavirus Vaccines Approved in China
Oral Pentavalent Reassortant Rotavirus Vaccine (Vero Cell)
RotaTeq (RV5), an oral pentavalent rotavirus vaccine, was approved in the United States in February 2006 and subsequently used in several European countries. This vaccine consists of five human-bovine (WC3) reassortant strains (G1, G2, G3, G4, and P1A[8]) and is in a three-dose series administered to infants aged 6–32 weeks. The first dose is given at 6–12 weeks of age, with subsequent doses spaced 4–10 weeks apart, and the third dose must be completed by 32 weeks of age. RotaTeq received WHO prequalification in 200819 and was launched in China market in 2018. According to data from Shanghai CDC, the procurement price for this vaccine in Shanghai is 285.5 CNY per dose.
IgA is considered the most acceptable laboratory parameter for assessing the immunogenicity of rotavirus vaccines. It is commonly used as a serological measure in clinical trials. Studies on natural rotavirus infections and vaccine trials have shown a correlation between serum rotavirus antibodies and vaccine protection. A randomized controlled trial in China reported a seroconversion rate of 89.4% for serum IgA following RotaTeq vaccination18. Another clinical trial evaluated the efficacy and safety of RotaTeq when co-administered with other vaccines, showing that RotaTeq provided 69.3% protection against RVGE of any severity caused by any serotype and 78.9% protection against severe RVGE caused by any serotype14. China local studies have consistently found that three doses of RotaTeq are highly effective against rotavirus-induced diarrhea. A study in Shanghai reported RotaTeq’s efficacy of 85% (95% CI: 50%–95%) in children aged 14 weeks to 4 years and 97% (95% CI: 83%–100%) in children aged 14 weeks to 2 years, primarily against G8P[8], G9P[8], and G2P[4] strains, which accounted for 78.95%, 18.42%, and 2.63% of prevalent strains, respectively36. In Beijing, the vaccine effectiveness (VE) of three doses of RotaTeq was 90.4% (95% CI: 28.8%–98.7%) against group A rotavirus diarrhea37.
A study conducted in Chengdu found that the introduction of RotaTeq led to a delayed onset of the rotavirus season, a shortened epidemic duration (from 20 to 7 weeks), and a significantly reduced peak positivity rate38. Since its approval in China in 2018, post-marketing surveillance data have shown no severe adverse events associated with large-scale RotaTeq vaccination19,20. Furthermore, China’s Adverse Events Following Immunization (AEFI) surveillance data for 2020 reported a total of 226,320 AEFI cases, with an overall AFEI reporting rate of 40.94 per 100,000 doses, and 14.37 per 100,000 doses for RotaTeq (RV5 in the Figure) 29.
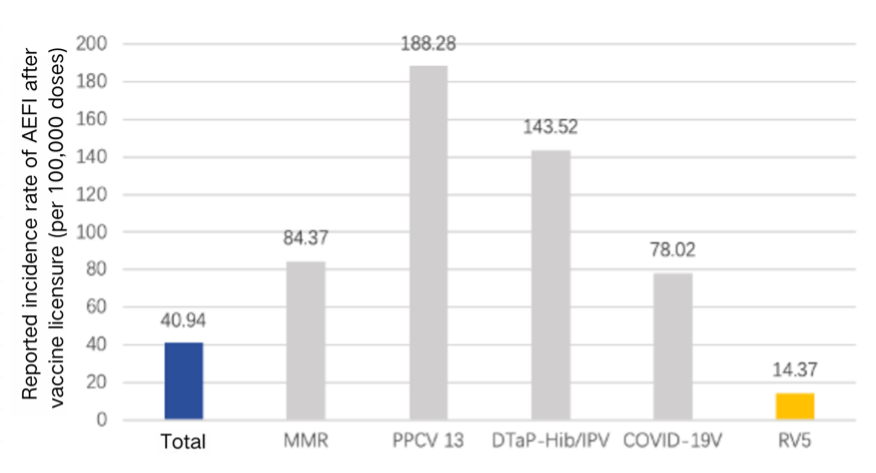
Source: Zhang LN, Li KL, Li Y, et al. Surveillance of adverse events following immunization in China,2020. Chinese Journal of Vaccines and Immunization. 2022;28(2):208–218. DOI:10.19914/j.CJVI.2022041
Oral Rotavirus Live Vaccine
The rotavirus vaccine developed by the Lanzhou Institute of Biological Products in China, known as LLR, is marketed under the brand name “LuoTeWei.” LLR was introduced in China in 2001 but has limited use since rotavirus vaccine has not been included in the national immunization program. The procurement price for LLR in Shanxi Province is 138 CNY per dose in 2024.
Since its introduction in 2001, over 50 million doses of LLR have been administered. Clinical evidence shown that LLR provides certain extent of protection against human rotavirus infections. Previous studies in China have reported lower adverse event rates in LLR recipients compared to control groups, with no cases of intussusception or death, indicating a good safety profile of the vaccine. The incidence of diarrhea was lower in the LLR group than in the control group21-24. Prospective cohort studies and meta-analyses have shown that LLR provides 69%–72% protection against RVGE and severe RVGE, comparable to the efficacy of rotavirus vaccines produced by GlaxoSmithKline and Merck21,22. Retrospective studies based on case data and vaccination records have found that one dose of LLR provides protection for children under 5 years of age, particularly against severe RVGE. These studies generally recommend completing the full vaccination schedule as early as possible to maximize protection39-41. One study in Beijing from 2015 to 2017 reported adjusted vaccine effectiveness (VE) estimates of 36.2% (95% CI: 4.7%–57.3%) and -1.6% (95% CI: -224.5%–68.2%) for children aged 2–35 months and 36–59 months, respectively42. A study in Guangzhou from 2002 to 2004 found that the effectiveness of 1 dose LLR was 60.0% in children aged 2–11 months, 80.9% in those aged 12–23 months, and 50% in those aged 24–35 months43.
A study in Shaanxi Province found that Rotavirus vaccination (LLR or RotaTeq) significantly reduced the duration and frequency of vomiting in hospitalized children under 5 years of age44. Another study using surveillance data from four cities in Guangdong Province conducted a test-negative case-control study to compare the effectiveness of LLR and RotaTeq against RVGE in hospitalized children from 2020 to 2023. The results showed that both vaccines effectively prevented RVGE, including cases caused by the G8P[8] genotype. Three doses of RotaTeq provided strong protection, while two doses of LLR were also an effective strategy for preventing rotavirus infections25.
Table 4.2 Comparison of LLR and RotaTeq Vaccine Efficacy by Dose and Severity
| Vaccine | Doses | Efficacy Against Any RVGE (%) | Efficacy Against Severe RVGE (%) |
| RotaTeq | 1 | 51.7 | 67.2 |
| 2 | 37.6 | 74 | |
| 3 | 64.1 | 86.6 | |
| LLR | 1 | 38.7 | 57.7 |
| 2 | 74.6 | 73.4 | |
| 3 | 58.8 | -27.8 |
Oral Trivalent Reassortant Rotavirus Vaccine (Vero Cell)
LLR3, a human-lamb reassortant trivalent rotavirus vaccine developed by the Lanzhou Institute of Biological Products, contains G2, G3, and G4 serotypes. A randomized, double-blind, placebo-controlled multicenter study demonstrated that LLR3 has good immunogenicity and protective efficacy against RVGE of any severity RVGE, severe RVGE, and hospitalizations caused by any serotype in Chinese infants14. LLR3 also showed cross-protection against other RV serotypes, particularly G9, with an efficacy of 70.3% (95% CI: 59.9%–77.9%) against severe RVGE caused by G9. Clinical trials indicated that LLR3 is safe for healthy children aged 2–35 months, with an adverse effect rate of 21.43%. Common adverse reactions included fever, vomiting, and diarrhea, with rates similar to other oral rotavirus vaccines, and no systemic severe adverse reactions were observed . LLR3 was approved for use in China in 202323. In 2025, the procurement price of LLR3 is 218 CNY per dose in Xinjiang Autonomous Region.
Rotavirus Vaccines in Development
RV3-BB Vaccine
Among the oral rotavirus vaccines in development, the most ready candidate is RV3-BB, developed by PTBioFarma in Indonesia. This vaccine is based on a naturally attenuated neonatal strain of RV G3P[6] and is currently in clinical trials3,24. Phase I trials have shown that RV3-BB is well-tolerated in adults, children, and neonates, with good immunogenicity observed in neonates after three doses25.
Oral Hexavalent Recombinant Rotavirus Vaccine (HRV6)
HRV6, developed by the Wuhan Institute of Biological Products, contains six serotypes: G1, G2, G3, G4, G8, and G9, covering 99.6% of the G serotypes of group A rotavirus5. Early clinical trials of HRV6 demonstrated good tolerance in both adults and infants, with promising immunogenicity in infants26. A randomized, double-blind, placebo-controlled, multicenter Phase III clinical trial was conducted in Hebei, Hunan, Zhejiang Province, and Guangxi Zhuang Autonomous Region. The results showed no significant differences in the incidence of adverse events and serious adverse events between the HRV6 group and the placebo group27.
Overview of Rotavirus Vaccines in Development in China
Table 4.3 Overview of Rotavirus Vaccines in Development in China
| Vaccine Name | Manufacturer | Covered Serotypes | Registration Category | Development Progress |
| Tri-valent Rotavirus Gene Reassortant Vaccine | Lanzhou Institute of Biological Products | G2, G3, G4 | 1 | Production application* |
| Oral Hexavalent Recombinant Rotavirus Live Vaccine (Vero Cell) | Wuhan Institute of Biological Products | G1, G2, G3, G4, G8, G9 | 1 | Phase III completed, Market application submitted |
| Human Rotavirus Live Attenuated Vaccine | GSK | G1P[8] | 3.1 | Phase III completed |
| Reassortant Tri-valent Rotavirus Subunit Vaccine | Micocon Bio | P[4], P[6], P[8] | 1.2 | Phase II |
| Monovalent Rotavirus Inactivated Vaccine | Kunming Institute of Biological Products | G1P[8] | – | Phase II |
| Oral Hexavalent Human-Cow Reassortant RV Live Attenuated Vaccine (Vero Cell) | Sinovac Biotech | G1, G2, G3, G4, G9, P1A[8] | 1 | Phase I |
| Oral Pentavalent Recombinant Rotavirus Live Vaccine (Vero Cell) | Kangtai Biotech | G1, G2, G3, G4, G9 | 3.2 | Phase I |
| Rotavirus Inactivated Vaccine (Vero Cell) | Chinese Academy of Medical Sciences, Institute of Biology | G1, G2, G3, G4, G9 | 1 | Phase I |
| Rotavirus Inactivated Vaccine | Zhifei Biological | G1P[8] | 1 | Phase I |
| Freeze-Dried Quadrivalent Oral Rotavirus Live Vaccine (FRhL-2 Cell) | Bravovax Co. | – | 1 | Approved for clinical use |
| Wa-VP4* Candidate Rotavirus Vaccine | Xiamen Innovax Biotech | – | – | Preclinical |
| Rotavirus mRNA-LNP Vaccine | Chinese Academy of Medical Sciences, Institute of Biology | – | – | Preclinical |
Data Source: Company announcements, Huajing Industry Research Institute, and the Clinical Research Database of the National Medical Products Administration.
*Approved for domestic market in April 2023.
Overview of Rotavirus Vaccines in Development in Other Countries
Table 4.4 Overview of Rotavirus Vaccines in Development Internationally
| Vaccine Name | Manufacturer/Developer | Vaccine Characteristics | Covered Serotypes | Development Progress |
| RV3-BB | PT BioFarma, Bandung, Indonesia | Based on human neonatal live-attenuated strain; neonatal (“birth dose”) and infant schedules being evaluated | G3P[6] | Phase 2/3; Phase 2b completed |
| VP8 Subunit Protein Vaccine | PATH Rotavirus Vaccine Program, USA | Subunit vaccine based on recombinant proteins; Parenteral administration being evaluated | Trivalent truncated VP8: P[4], P[6], P[8] | Phase 3 |
| Tetravalent UK-BRV | Shanta Biotechnics | Based on live-attenuated bovine-human reassortant strain | G1-4 | Phase 3, development abandoned |
| Pentavalent UK-BRV | Instituto Butantan, Brazil | Based on live-attenuated bovine-human reassortant strain | G1-4, G9 | Phase 1 |
| Hexavalent UK-BRV* | Wuhan Institute of Biological Products, China | Based on live-attenuated bovine-human reassortant strain | G1-4, G8, G9 | Phase 2/3 |
| Inactivated G1P[8] Vaccine | CDC, USA | Heat inactivated human strain; Parenteral administration being evaluated | G1P[8] | Preclinical; Animal studies |
| VP6-Norovirus VLP | University of Tampere | Subunit vaccine based on virus-like particles; Parenteral administration being evaluated | N/A; VP6 protein | Preclinical; Animal studies |
| Expressed V6 Protein | Cincinnati Children’s Hospital Medical Center | Subunit vaccine based on recombinant proteins; Parenteral administration being evaluated | N/A; VP6 protein | Preclinical; Animal studies |
| VLP VP2/6(/7) | Baylor College of Medicine | Subunit vaccine based on virus-like particles; Parenteral administration being evaluated | N/A; VP2/6/7 protein | Preclinical; Animal studies |
Data Source: Cates, J., Tate, J. E., & Parashar, U. Rotavirus vaccines: progress and new developments. Expert Opinion on Biological Therapy 22, 423–432 (2022).28
*Chinese product.
It has been suggested that the next-generation injectable rotavirus vaccines may offer higher protective efficacy, or the combination of oral and injectable vaccines may enhance effectiveness. Furthermore, the study emphasizes that co-administration of the next-generation injectable rotavirus vaccine with the DTP vaccine may effectively improve vaccination coverage and is considered a cost-effective choice. The study supports the necessity of developing injectable rotavirus vaccines45.
Content Editor: Siqi Jin, Ziqi Liu
Page Editor:Ziqi Liu
References
- Vaccine in National Immunization Programme Update. https://cdn.who.int/media/docs/default-source/immunization/hpv/vaccineintrostatus.pdf
- Burnett, E., Parashar, U. D. & Tate, J. E. Real-world Effectiveness of Pentavalent Rotavirus Vaccine in Shanghai of rotavirus vaccines, 2006–19: a literature review and meta-analysis. The Lancet Global Health 8, e1195–e1202 (2020).
- Cárcamo-Calvo, R., Muñoz, C., Buesa, J., Rodríguez-Díaz, J. & Gozalbo-Rovira, R. The Rotavirus Vaccine Landscape, an Update. Pathogens 10, 520 (2021).
- Clark, A. et al. Efficacy of live oral rotavirus vaccines by duration of follow-up: a meta-regression of randomised controlled trials. The Lancet Infectious Diseases 19, 717–727 (2019).
- Rotavirus Gastroenteritis Expert Consensus Writing Group. Expert consensus on immunoprevention of rotavirus gastroenteritis in children (2024 edition). Chinese Journal of Preventive Medicine. 2024;58(0):1-33. DOI:10.3760/cma.j.cn112150-20231220-00472
- National Medical Products Administration. Data query : Registration No. S20230022. https://www.nmpa.gov.cn/datasearch/search-info.html?nmpa=aWQ9YjFjOWVlMTQyOGJhMzkyZTFmMTdiN2ZkYjk0M2M1ZjQmaXRlbUlkPWZmODA4MDgxODNjYWQ3NTAwMTg0MDg4MWY4NDgxNzlm.
- VIEW-hub. (n.d.). Rotavirus vaccine. Retrieved October 11, 2024, from https://view-hub.org/vaccine/rota
- https://www.cdc.gov/vaccines/vpd/rotavirus/hcp/index.html
- https://www.path.org/our-impact/media-center/india-made-rotavirus-vaccine-achieves-world-health-organization-prequalification/
- https://www.path.org/our-impact/media-center/global-rotavirus-vaccine-options-expand-world-health-organization-prequalification-new-vaccine-india/
- Lanzhou Institute of Biological Products Co., Ltd. Package insert of Reassortant Rotavirus Vaccine, live, Oral, Trivalent (Vero Cell) . Available from: https://www.vacmic.com/htm/20246/13_2861.htm
- Giaquinto, C. et al. Summary of effectiveness and impact of rotavirus vaccination with the oral pentavalent rotavirus vaccine: A systematic review of the experience in industrialized countries. Human Vaccines 7, 734–748 (2011).
- Lawrence, J. et al. Safety and immunogenicity of pentavalent rotavirus vaccine in a randomized, double-blind, placebo-controlled study in healthy elderly subjects. Human Vaccines & Immunotherapeutics 10, 2247–2254 (2014).
- Xia, S. et al. Efficacy, immunogenicity and safety of a trivalent live human-lamb reassortant rotavirus vaccine (LLR3) in healthy Chinese infants: A randomized, double-blind, placebo-controlled trial. Vaccine 38, 7393–7400 (2020).
- Wei YH, et al. Meta-analysis of the protective effect and safety of RotaTeq vaccine against rotavirus gastroenteritis in children in high mortality areas in the world. Chinese Journal of Experimental and Clinical Virology. 2023;37:106–111.
- Desselberger, U. Differences of Rotavirus Vaccine Effectiveness by Country: Likely Causes and Contributing Factors. Pathogens 6, 65 (2017).
- Dadonaite, B., Ritchie, H. & Roser, M. Rotavirus vaccine – an effective tool that prevents children dying from diarrhea. Our World in Data (2024).
- Mo, Z. et al. Immunogenicity of pentavalent rotavirus vaccine in Chinese infants. Vaccine 37, 1836–1843 (2019).
- Huang WB, Guo WF, Sun YS, Zhu YQ. Safety investigation of oral pentavalent reassortant live attenuated rotavirus vaccine in infants and young children in Conghua District, Guangzhou. China Rural Health. 2020;12:75–77.
- Fang T, Zhao XF, Han HT, Ni HX, Zhang L. Active surveillance of adverse events following immunization with pentavalent live human-bovine reassortant rotavirus vaccine among 6–12-week-old infants in Ningbo city. Chinese Journal of Vaccines and Immunization. 2021;27:580–583.
- Li MQ, Lü BJ, Shen PY. The meta-analysis of protective effect and safety of oral rotavirus vaccine (live). Chinese Journal of Disease Control & Prevention. 2015;19:1038–1041, 1056.
- Cao B, Wang XH, You ZY, Tan SQ, Hu GF. The meta-analysis of vaccine effectiveness of Lanzhou lamb rotavirus vaccine. Chinese Journal of Disease Control & Prevention. 2013;17(3):203–207. DOI:10.3760/cma.j.issn.1673-4092.2013.03.003.
- Xia S, Du J, Su J, et al. Efficacy, immunogenicity and safety of a trivalent live human-lamb reassortant rotavirus vaccine (LLR3) in healthy Chinese infants: A randomized, double-blind, placebo-controlled trial. Vaccine. 2020;38(46):7393-7400. doi:10.1016/j.vaccine.2020.04.038
- Glass, R. I., Tate, J. E., Jiang, B. & Parashar, U. The Rotavirus Vaccine Story: From Discovery to the Eventual Control of Rotavirus Disease. J Infect Dis 224, S331–S342 (2021).
- Yi, Y., Liu, J., Zhang, Y. et al. Effectiveness of Lanzhou Lamb Rotavirus Vaccine and RotaTeq Against Hospitalized Rotavirus Infections Among Children During 2020-2023 in Guangdong Province, China: A Test-Negative Case-Control Study. Infect Dis Ther 13, 2301–2317 (2024). https://doi.org/10.1007/s40121-024-01040-y
- At Thobari, J. et al. Safety and immunogenicity of human neonatal RV3 rotavirus vaccine (Bio Farma) in adults, children, and neonates in Indonesia: Phase I Trial. Vaccine 39, 4651–4658 (2021).
- Safety and immunogenicity of a novel oral hexavalent rotavirus vaccine a phase I clinical trial.pdf.
- Wu, Z. et al. Efficacy, safety and immunogenicity of hexavalent rotavirus vaccine in Chinese infants. Virologica Sinica 37, 724–730 (2022).
- Cates, J., Tate, J. E. & Parashar, U. Rotavirus vaccines: progress and new developments. Expert Opin Biol Ther 22, 423–432 (2022).
- Zhang LN, Li KL, Li Y, et al. Surveillance of adverse events following immunization in China, 2020. Chinese Journal of Vaccines and Immunization. 2022;28(2):208–218. DOI:10.19914/j.CJVI.2022041.
- Bencina G, Costantino C, Mameli C, Sabale U, Murtagh J, Newman R, Ahern A, Bhaila R, Sanchez AO, Martinon-Torres F, Carias C. Real-world impact of rotavirus vaccination in European healthcare settings: a systematic literature review. Expert Rev Vaccines. 2022 Aug;21(8):1121-1136. doi: 10.1080/14760584.2022.2075851. Epub 2022 Jun 16. PMID: 35708263.
- Sun ZW, Fu Y, Lu HL, Yang RX, Goyal H, Jiang Y, Xu HG. Association of Rotavirus Vaccines With Reduction in Rotavirus Gastroenteritis in Children Younger Than 5 Years: A Systematic Review and Meta-analysis of Randomized Clinical Trials and Observational Studies. JAMA Pediatr. 2021 Jul 1;175(7):e210347. doi: 10.1001/jamapediatrics.2021.0347. Epub 2021 Jul 6. PMID: 33970192; PMCID: PMC8111566.
- Gidengil C, Goetz MB, Newberry S, Maglione M, Hall O, Larkin J, Motala A, Hempel S. Safety of vaccines used for routine immunization in the United States: An updated systematic review and meta-analysis. Vaccine. 2021 Jun 23;39(28):3696-3716. doi: 10.1016/j.vaccine.2021.03.079. Epub 2021 May 25. PMID: 34049735.
- Pereira P, Benninghoff B, Moerman L. Systematic literature review on the safety and immunogenicity of rotavirus vaccines when co-administered with meningococcal vaccines. Hum Vaccin Immunother. 2020 Nov 1;16(11):2861-2872. doi: 10.1080/21645515.2020.1739485. Epub 2020 Apr 16. PMID: 32298219; PMCID: PMC7746238.
- Raboba JL, Rahajamanana VL, Rakotojoelimaria HE, Masembe YV, Martin PR, Weldegebriel GG, Diallo AO, Burnett E, Tate JE, Parashar UD, Mwenda JM. Monovalent rotavirus vaccine effectiveness and long-term impact among children< 5 years old in Antananarivo, Madagascar, 2010–2022. Vaccine. 2024 Dec 2;42(26):126321.
- Ma W, Wei Z, Guo J, et al. Effectiveness of Pentavalent Rotavirus Vaccine in Shanghai, China: A Test-Negative Design Study. J Pediatr. 2023;259:113461. doi:10.1016/j.jpeds.2023.113461
- Tian, Y., Shen, L., Li, W., Yan, H., Fu, J., Liu, B., Wang, Y., Jia, L., Li, G., Suo, L., Zhang, D., Gao, Z., & Wang, Q. (2024). Major changes in prevalence and genotypes of rotavirus diarrhea in Beijing, China after RV5 rotavirus vaccine introduction. Journal of medical virology, 96(5), e29650. https://doi.org/10.1002/jmv.29650
- Xiao G, Zhu T, Wang Z, et al. Pentavalent Rotavirus Vaccine Coverage and Trends in Rotavirus Detection Before and After This Vaccination in Chengdu, China. Pediatr Infect Dis J. 2024;43(11):e397-e399. DOI: 10.1097/INF.0000000000004441
- Li J, Zhang Y, Yang Y, Liang Z, Tian Y, Liu B, Gao Z, Jia L, Chen L, Wang Q. Effectiveness of Lanzhou lamb rotavirus vaccine in preventing gastroenteritis among children younger than 5 years of age. Vaccine. 2019 Jun 12;37(27):3611-6.
- Fu C, Wang M, Liang J, He T, Wang D, Xu J. Effectiveness of Lanzhou lamb rotavirus vaccine against rotavirus gastroenteritis requiring hospitalization: a matched case-control study. Vaccine. 2007 Dec 17;25(52):8756-61.
- Fu C, He Q, Xu J, Xie H, Ding P, Hu W, Dong Z, Liu X, Wang M. Effectiveness of the Lanzhou lamb rotavirus vaccine against gastroenteritis among children. Vaccine. 2012 Dec 17;31(1):154-8.
- Li J, Zhang Y, Yang Y, Liang Z, Tian Y, Liu B, Gao Z, Jia L, Chen L, Wang Q. Effectiveness of Lanzhou lamb rotavirus vaccine in preventing gastroenteritis among children younger than 5 years of age. Vaccine. 2019 Jun 12;37(27):3611-6.
- Fu C, Wang M, Liang J, He T, Wang D, Xu J. Effectiveness of Lanzhou lamb rotavirus vaccine against rotavirus gastroenteritis requiring hospitalization: a matched case-control study. Vaccine. 2007 Dec 17;25(52):8756-61.
- Zhu N, Zhang Y, Chen S, Feng X, Li H, Hu WJ, Zhang C, Cao L, Zhang SB. Effectiveness of rotavirus vaccine in preventing rotavirus infection and clinical symptoms among hospitalized children under five years of age with diarrhea. Chinese Journal of Vaccines and Immunization. 2024;30(4):447–450.
- Hausdorff WP, Price J, Debellut F, Mooney J, Torkelson AA, Giorgadze K, Pecenka C. Does anybody want an injectable rotavirus vaccine, and why? Understanding the public health value proposition of next-generation rotavirus vaccines. Vaccines. 2022 Jan 20;10(2):149.
- Li J, Zhang Y, Yang Y, et al. Effectiveness of Lanzhou lamb rotavirus vaccine in preventing gastroenteritis among children younger than 5 years of age. Vaccine. 2019;37(27):3611-3616. doi:10.1016/j.vaccine.2019.03.069
