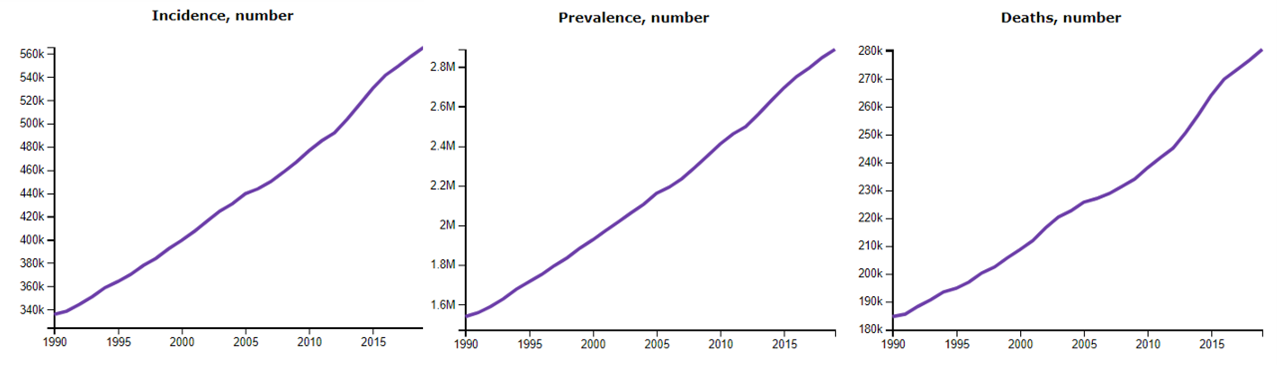
Cervical cancer is the fourth most common cancer in women worldwide. The number of new cases and deaths from cervical cancer has been increasing globally over the past two decades (Figure 1). Cervical cancer is the leading cancer among women in 23 countries and the leading cause of cancer death among women in 36 countries. The disease burden of cervical cancer is unevenly distributed globally, with morbidity and mortality in low- and middle-income countries being 1.7 and 2.4 times higher than in high-income countries respectively [1]. According to the International Agency for Research on Cancer (IARC), the global disease burden of cervical cancer is projected to increase if no further action is taken, with the number of new cervical cancer cases per year increasing from 570,000 to 700,000 and the number of deaths per year projected to increase from 311,000 to 400,000 between 2018 and 2030 [1, 2].
Figure 1. global number of incidence, prevalence, and deaths of cervical cancer, 1990-2020
Incidence
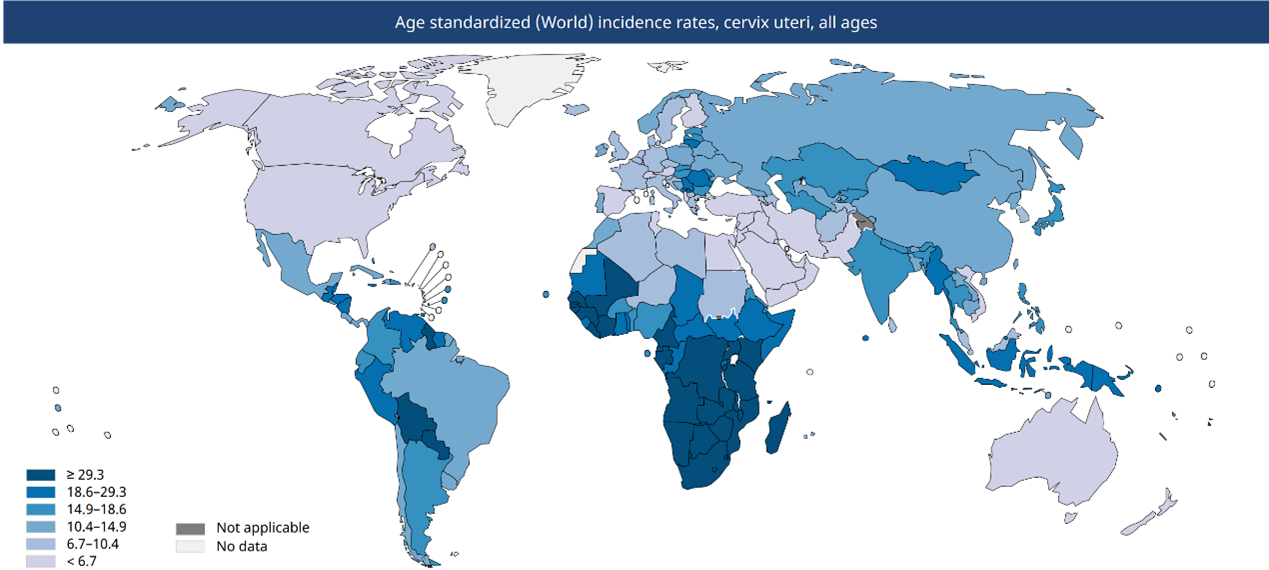
Cervical cancer is the fourth most common cancer in women worldwide, after breast, colorectal and lung cancers. According to data from the Global Cancer Observatory from 185 countries, it is predicted that there will be nearly 604,000 new cases of cervical cancer globally in 2020, accounting for 6.5% of all female cancer cases, which is equivalent to 13.3 cases per 100,000 women per year globally[2]. The incidence of cervical cancer varies widely, with approximately 84% of new cases globally coming from low- and middle-income countries (Figure 2). According to the Global Cancer Data 2020 report, West Asia has the lowest age-standardized incidence rate (approximately 4.1 per 100,000 females) and East Africa has the highest rate (approximately 40.1 per 100,000 females) [1]. Population-based cervical cancer incidence rates also increase with decreasing of the country’s Human Development Index (HDI). In countries with a high HDI (greater than 0.8), there is an average of 9.6 new cases per 100,000 females per year, whereas in countries with a lower HDI, the incidence rate rises to 26.7 new cases per 100,000 females per year [1].
Figure 2: Global age-standardized incidence of cervical cancer by country, 2020
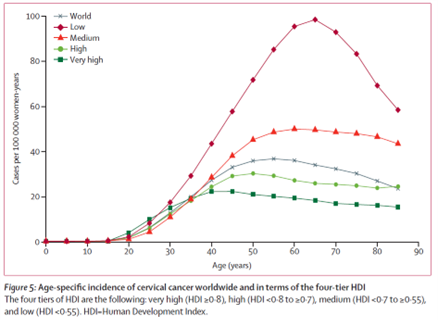
The incidence of cervical cancer varies among women of different ages, with the incidence rising after the age of 25 years, reaching a maximum around the age of 40 in countries with a very high HDI. However, the number of incidence rise significantly in countries with a low NHI until it reaches a maximum around the age of 60 [1] (Figure 3).
Figure 3. Age-specific incidence of cervical cancer worldwide and in terms of four tier HDI
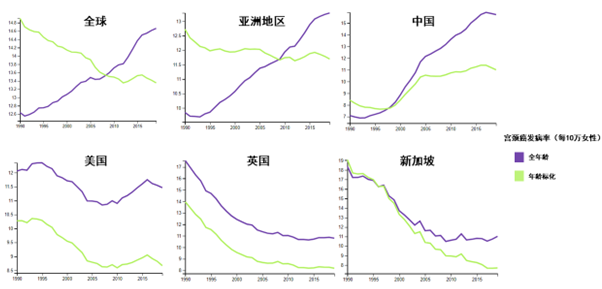
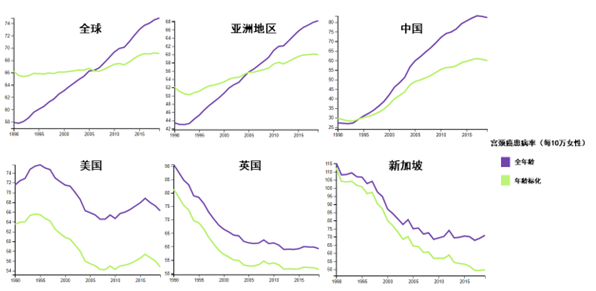
Although the cervical cancer incidence rate has been increasing over the past 20 years, the global age-standardized incidence of cervical cancer has shown a decreasing trend, thanks to economic and social development, improved sanitation, and advocacy and action to eliminate sexually transmitted infections (Figure 4). Through interventions such as HPV vaccination and cervical cancer screening, the incidence of cervical cancer in high-income countries such as the United States, the United Kingdom, Australia, Singapore, Denmark, and Japan has shown a downward trend from year to year, which further demonstrates that cervical cancer can be effectively prevented.
Figure 4. Incidence of cervical cancer in women globally and in selected region and countries, 1990-2015
Prevalence
The absolute number of cases of cervical cancer is increasing globally, but the growth of age-standardized prevalence has slowed down in recent years (Figure 5). According to the Global Burden of Disease Project, about 2,887,000 women of all ages worldwide have cervical cancer, and the age-standardized prevalence of cervical cancer is about 74.9 per 100,000 women, with one-third of the cervical cancer patients coming from China and India [1].
Figure 5. Prevalence of cervical cancer in women globally and in selected region and countries, 1990-2015
Mortality rate
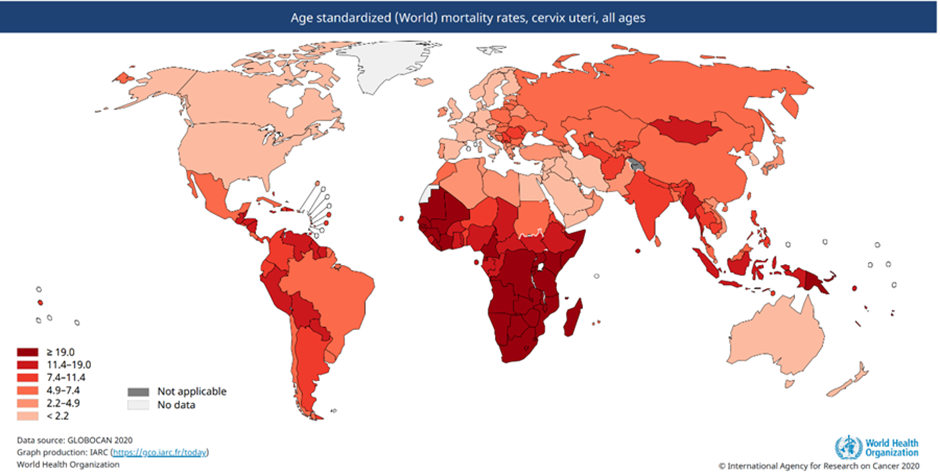
Cervical cancer is the fourth leading cause of cancer deaths in women, after breast, lung and colorectal cancers. It is estimated that 342,000 women will die globally from cervical cancer in 2020, with an age-standardized mortality rate of 7.3 deaths per 100,000 women per year[1] (Figure 6A).
Figure 6A. Cervical cancer age-standardized (World) mortality rates, 2020
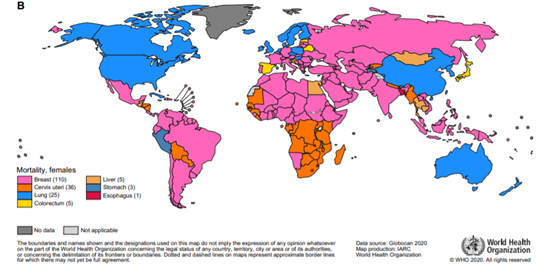
About 88% of these deaths globally occur in low- and middle-income countries, where about 1.3% of women die of cervical cancer before the age of 75 years. Cervical cancer is the leading cause of cancer deaths in women in 36 countries worldwide (Figure 6B). The mortality rate from cervical cancer differs from regions, which exists both between and within countries. In countries with a high HDI, the average number of deaths from cervical cancer is 3 per 100,000 women, whereas in countries with a low HDI this figure can rise to 26.7 deaths per 100,000 women [1]. Mortality from cervical cancer also varies within countries. In the United States, for example, cervical cancer mortality rates are twice as high in lower-income regions as in more economically developed regions [2]. This significant regional variation stems primarily from inequalities in the extent of risk factor exposure, level of medical care, and access to screening and effective therapeutic interventions. In low- and middle-income countries, where preventive measures are limited, diagnosis is often made after the disease has progressed to an advanced stage, and access to treatment for advanced cervical cancer may be very limited, resulting in higher cervical cancer mortality rates in resource-constraint regions.
Figure 6B. Top types of female cancer mortality in different countries, 2020
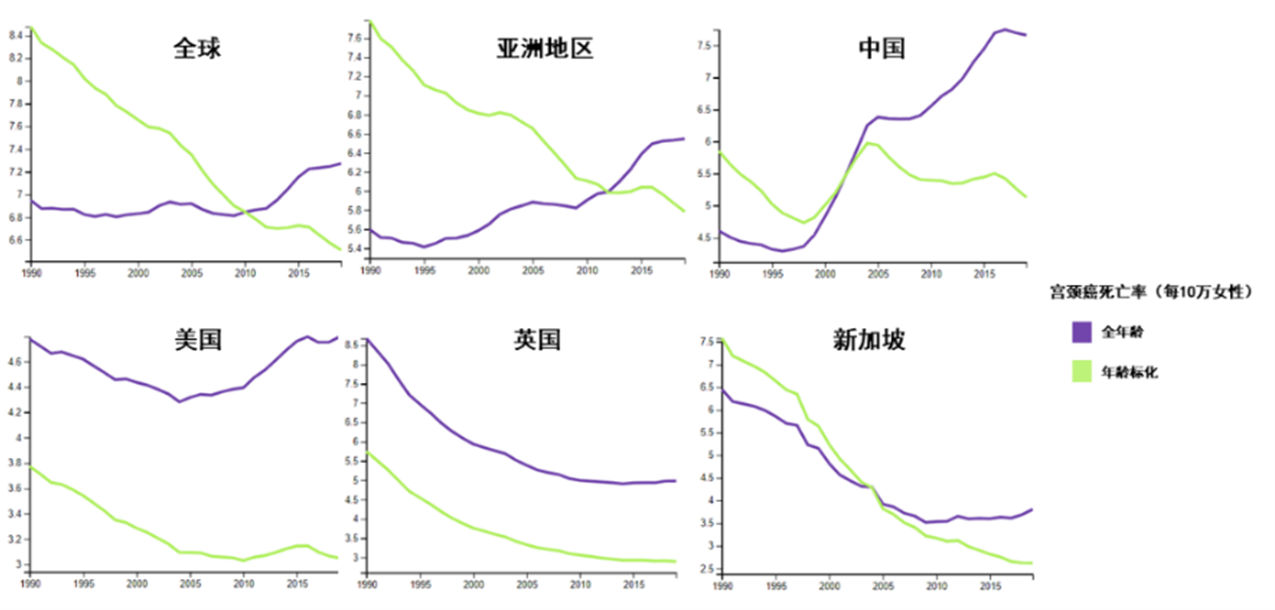
Although cervical cancer deaths have been the fourth highest of all cancers, the total number of cervical cancer deaths as a percentage of all cancer deaths has decreased from 8.2% in 2008 to 7.7% in 2020 [2]. Age standardized mortality rates have also continued to decrease over the past 30 years (Figure 7).
Figure 7. Mortality rate of cervical cancer in women globally and in selected region and countries, 1990-2015
Content Reviewer: Kelly Hunter, Zhangyang Pan
References:
- Arbyn M, Weiderpass E, Bruni L, de Sanjosé S, Saraiya M, Ferlay J, Bray F: Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. The Lancet Global Health 2020, 8(2):e191-e203.
- Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Piñeros M, Znaor A, Bray F: Cancer statistics for the year 2020: An overview. International Journal of Cancer 2021.
